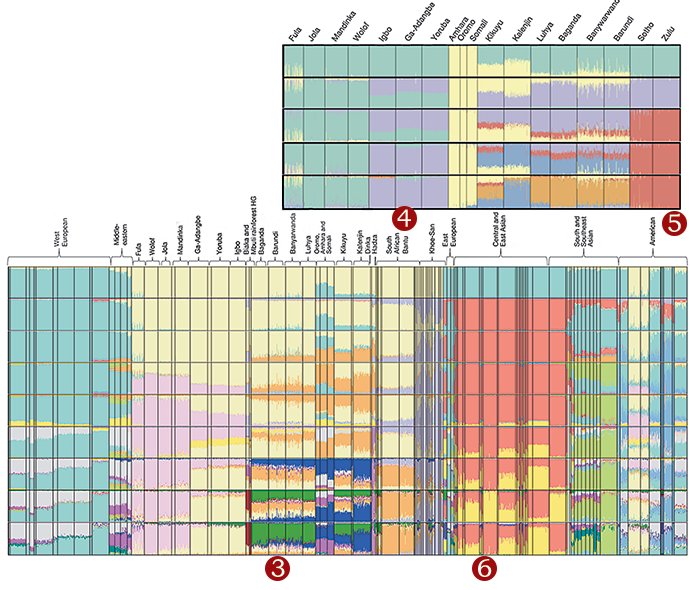
1. In 2014, Deepti Gurdasani, a genetic epidemiologist at the Wellcome Sanger Institute in England, coauthored a paper in Nature on human genetic variation in Africa, from which this image is taken. A recent study had found that DNA from people of European descent made up 96 percent of genetic samples worldwide, reflecting the historical tendency among scientists and doctors to view the male, European body as a global archetype. “There wasn’t very much data available from Africa at all,” Gurdasani told me. To help rectify the imbalance, her research team collected samples from eighteen African ethnolinguistic groups across the continent—such as the Kalenjin of Uganda and the Oromo of Ethiopia—most of whom had not previously been included in genomic research. They analyzed the data using an admixture algorithm, which visualizes the statistical genetic differences among groups by representing them as color clusters. The top chart shows genetic differences among the sampled African populations, in increasing degrees of granularity from top to bottom, and the bottom chart shows how they compare with ethnic groups in the rest of the world. The areas where the colors mix and overlap imply that groups commingled. The Yoruba, for instance, show remarkable homogeneity—their column is almost entirely green and purple—while the Kalenjin seem to have associated with many populations across the continent.
2. Fifteen years earlier, scientists at a medical center in Dallas had begun searching for people with mutations in a gene known as PCSK9. Previous studies had found that a mutation that activated this gene leads to excessive cholesterol in the blood, causing waxy, yellow clumps to accumulate under the skin. When a mutation inhibited the expression of PCSK9, however, cholesterol levels were lower, even in people with lifestyle risks such as smoking cigarettes or eating high-fat foods. For researchers working in the emerging field of genetic medicine, PCSK9 was a promising lead. If they could find people with the inactive mutation on both copies of the gene, they might be able to develop a safe medication to prevent coronary heart disease, which is responsible for one in eight deaths in the United States. But the search would not be easy. The inactive PCSK9 mutation was most common in people of African ancestry. In the available data, scientists could find only one person who carried a double inactive mutation of PCSK9: a thirty-two-year-old, African-American aerobics instructor in Dallas. As they had hoped, the instructor had astoundingly low cholesterol levels—around one seventh the amount of the average adult. A year later, researchers in South Africa identified another case—a twenty-one-year-old woman, who was in a maternity ward in Zimbabwe—that confirmed the Dallas findings. Studying her genome led to the development of two effective drugs for managing cholesterol.
3. The reason African genomes are so important in drug discovery has to do with the history of human evolution and migration. According to the “Out of Africa” model, when small groups of Homo sapiens began to leave the continent around one hundred thousand years ago, they passed through a population bottleneck. The migrant communities had far fewer people with whom they could reproduce, which greatly diminished the gene pool in these geographically dispersed populations. To this day, people of African descent—whose ancestors did not pass through the population bottleneck—carry more genetic diversity than people of non-African ancestry. African genomes, therefore, offer researchers a depth of genetic information that non-African genomes simply don’t have. In the years after the PCSK9 studies, which over-sampled people of African descent to increase the chances of finding the relevant mutation, many prominent geneticists realized that progress in the field would slow dramatically unless general sampling practices were expanded to include African ancestral groups. Genetic databases would need to be radically diversified.
4. Researchers founded diversity initiatives, including the 1000 Genomes Project, which sampled people across five continents, and All of Us, which focused on minority communities in the United States. These projects claimed to serve the interests of under-sampled groups, but for some they evoked a fraught history of medical exploitation. Many African Americans remembered the story of Henrietta Lacks, a black woman whose cancer cells were taken and used, without her consent, to develop the polio vaccine in the 1950s. Unethical research on non-white subjects has continued into the twenty-first century. In 2010, an international team of geneticists published an article analyzing blood samples from four elders of the San people, hunter-gatherers who are indigenous to southern Africa, without obtaining proper authorization. The Working Group of Indigenous Minorities in Southern Africa wrote a letter to the journal excoriating the researchers, who, they said, had displayed “absolute arrogance, ignorance, and cultural myopia.” Gurdasani believes that some research institutes and pharmaceutical companies use the issue of diversity to justify a neocolonial approach to sampling—plundering the genomes of Africa. “They are interested in studying genetic diversity in Africa so they can develop drugs that can be marketed across the world,” she said.
5. Gurdasani and her team at the Sanger Institute were determined to do things differently. They obtained consent on a village-by-village basis and built clinics to ensure that people who were diagnosed with genetic conditions during the sampling process had access to follow-up treatment. Gurdasani hoped to use the African data they had collected to develop a gene chip—a high-density assemblage of synthetic molecules on a solid surface the size of a postage stamp—that would allow researchers to examine African genomes in the lab. The scientists planned to consult with the relevant communities to ensure that they consented to, and would benefit from, any attempt to share the data derived from their genetic material. But in 2017 Sanger went ahead and produced seventy-five thousand chips in partnership with Thermo Fisher Scientific, a biotechnology company, before an agreement had been reached. “This was not a naïve mistake,” Gurdasani told me. “They probably thought that none of the African institutes or communities had the money or legal infrastructure to really challenge them. So they just did it.” Outraged, Gurdasani and three other scientists lodged a formal whistle-blower complaint. Emails and documents from that year strongly suggest that Sanger intended to manufacture the chips for commercial sale. But after a six-month investigation, outside counsel hired by the institute concluded that there had been no wrongful exploitation of scientific work. “There was never any attempt or proposal to attempt commercialisation of genetic material from African communities,” a Sanger spokesperson said.
6. Since then, the four whistle-blowers have left the institute—Gurdasani, who is now a researcher at Queen Mary University of London, maintains that she was fired. Stellenbosch University in South Africa, which was a partner in the project, requested that Sanger return the genome samples it had contributed from people of Nama ancestry. This type of data restitution has become increasingly common as a way for indigenous groups to resist exploitation. Since 2017, the National Centre for Indigenous Genomics in Australia has repatriated hundreds of blood samples taken from Aboriginal Australians; the Navajo Nation in the United States has had a moratorium on genetic research since 2002; and the San people have established their own code of ethics for use by medical researchers. Some geneticists worry that these protective efforts will hamper progress in medical genetics and ultimately hurt under-sampled communities. “I think it’s a massive mistake and a massive missed opportunity,” Carlos Bustamante, a professor of genetics at Stanford University, told me. “You don’t participate, you won’t benefit.” But Gurdasani believes that the responsibility lies with researchers and pharmaceutical companies to establish consent. What remains to be seen, she says, is whether the field of genetic medicine can diversify its research without resorting to the extractive logic of colonialism.




























































































